Purpose
To evaluate the potential of cone-beam-CT (CB-CT) guided adaptive radiotherapy (ART) for locally advanced non-small cell lung cancer (NSCLC) for sparing of surrounding organs-at-risk (OAR).
Materials and Methods
In 10 patients with locally advanced NSCLC, daily CB-CT imaging was acquired during radio- (n = 4) or radiochemotherapy (n = 6) for simulation of ART. Patients were treated with conventionally fractionated intensity-modulated radiotherapy (IMRT) with total doses of 60–66 Gy (pPlan) (311 fraction CB-CTs). OAR were segmented on every daily CB-CT and the tumor volumes were modified weekly depending on tumor changes. Doses actually delivered were recalculated on daily images (dPlan), and voxel-wise dose accumulation was performed using a deformable registration algorithm. For simulation of ART, treatment plans were adapted using the new contours and re-optimized weekly (aPlan).
Results
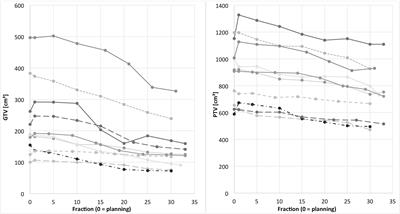
CB-CT showed continuous tumor regression of 1.1 ± 0.4% per day, leading to a residual gross tumor volume (GTV) of 65.3 ± 13.4% after 6 weeks of radiotherapy (p = 0.005). Corresponding PTVs decreased to 83.7 ± 7.8% (p = 0.005). In the actually delivered plans (dPlan), both conformity (p = 0.005) and homogeneity (p = 0.059) indices were impaired compared to the initial plans (pPlan). This resulted in higher actual lung doses than planned: V20Gy was 34.6 ± 6.8% instead of 32.8 ± 4.9% (p = 0.066), mean lung dose was 19.0 ± 3.1 Gy instead of 17.9 ± 2.5 Gy (p = 0.013). The generalized equivalent uniform dose (gEUD) of the lung was 18.9 ± 3.1 Gy instead of 17.8 ± 2.5 Gy (p = 0.013), leading to an increased lung normal tissue complication probability (NTCP) of 15.2 ± 13.9% instead of 9.6 ± 7.3% (p = 0.017). Weekly plan adaptation enabled decreased lung V20Gy of 31.6 ± 6.2% (−3.0%, p = 0.007), decreased mean lung dose of 17.7 ± 2.9 Gy (−1.3 Gy, p = 0.005), and decreased lung gEUD of 17.6 ± 2.9 Gy (−1.3 Gy, p = 0.005). Thus, resulting lung NTCP was reduced to 10.0 ± 9.5% (−5.2%, p = 0.005). Target volume coverage represented by conformity and homogeneity indices could be improved by weekly plan adaptation (CI: p = 0.007, HI: p = 0.114) and reached levels of the initial plan (CI: p = 0.721, HI: p = 0.333).
Conclusion
IGRT with CB-CT detects continuous GTV and PTV changes. CB-CT-guided ART for locally advanced NSCLC is feasible and enables superior sparing of healthy lung at high levels of plan conformity.

Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου
Σημείωση: Μόνο ένα μέλος αυτού του ιστολογίου μπορεί να αναρτήσει σχόλιο.